How Flow Measurements Provide Graft Patency Assurance
Acceptable Mean Flow Is Key:
PI Can Be Deceptive
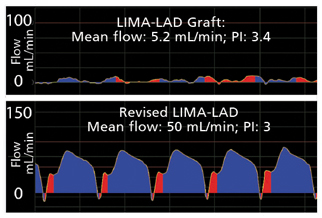
A 67-year-old male with single-vessel coronary artery disease underwent off-pump CABG. LIMA-LAD graft flow first measured 5.2 mL/min (PI: 3.4). The patient’s pulse and pressure appeared normal and the graft appeared functional, but the waveform exhibited a damped profile and atypical diastolization (top waveform). The surgeon decided to revise the graft. After revision, LIMA-LAD graft flow improved to 50 mL/min (PI: 3). The flow waveform (bottom) exhibited a classic LIMA-LAD profile. Note that the first PI was 3.4, the revised PI was 3.
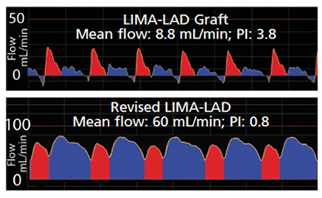
A 76-year-old male patient underwent coronary artery bypass grafting (CABG) surgery to bypass a lesion in the left anterior descending (LAD) artery utilizing a left internal mammary artery (LIMA) graft. Initial LIMA-LAD mean flow measured 8.8mL/min (PI: 3.8) (top waveform). The graft was revised. Following revision, LIMA-LAD mean flow improved to 60 mL/min (PI: 0.8) and was accompanied by a classic, diastolic dominant waveform profile (bottom waveform).
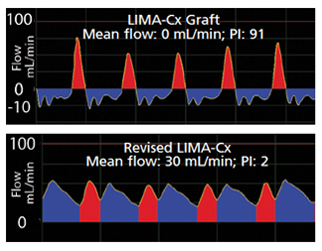
Zero Mean Flow Demands Revision of LIMA-Cx Graft
This case demonstrates a serious problem with a graft when flow measured 0 mL/min.
A 78-year-old female underwent single coronary bypass grafting to bypass a blocked circumflex (Cx) coronary artery with a LIMA graft. Flow first measured 0 mL/min (PI: 91) following anastomosis of the LIMA to the Cx. The flow waveform had a spiky systolic profile (top waveform). Revision was demanded. Following revision of the graft, mean graft flow improved to 30 mL/min (PI: 2), and the waveform exhibited a 1/3 to 2/3 systolic/diastolic profile. Zero mean flow was the determining factor in the decision to revise the graft.
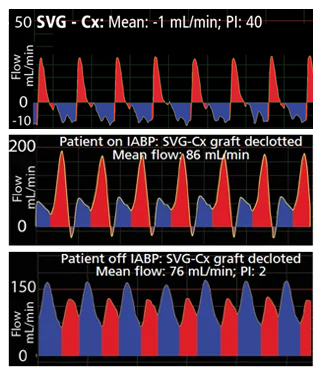
Zero Flow in SVG-Cx Graft Reveals Clot
This case demonstrates that IABP support does not significantly influence flow.
An 81-year-old male underwent CABG surgery to bypass a blocked circumflex (Cx) coronary artery. A harvested saphenous vein graft (SVG) was used to connect the aorta to the Cx distal to the lesion (top waveform). Following anastomosis of the SVG to the Cx, graft flow measured 0 mL/min, clearly indicating that there was a problem. Investigation revealed a clot in the graft. The patient was placed on IABP support. The graft was declotted and flow was remeasured with the patient still on IABP support. Flow measured 86 mL/min (middle waveform). When the IABP support was removed, graft flow measured 76 mL/min (PI: 2) indicating that the presence of an IABP did not significantly affect graft flow (bottom waveform).
Flow-based Patency Assurance
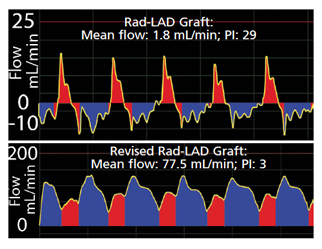
Poor Rad-LAD Graft Flow Triggers Graft Revision
This case demonstrates that poor flow signals a need for graft revision.
A 71-year-old male with single-vessel coronary artery disease underwent CABG surgery. A segment of the radial artery (Rad) was harvested and grafted proximally to the aorta and distally to the LAD. Initial Rad-LAD mean flow measured 1.8 mL/min (PI: 29) indicating that revision of the graft was warranted (top waveform). After revision, graft flow improved to 77.5 mL/ min (PI: 3). The flow was accompanied by a repetitive systolic/diastolic waveform profile (bottom waveform).
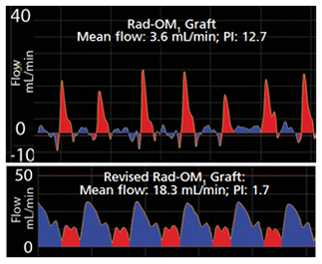
Low Mean Flow Spurs Rad-OM1 Graft Revision
Case demonstrates that poor flow in one out of four grafts signals need for graft revision in that one graft.
A 48-year old male with multi-vessel coronary artery disease underwent quadruple CABG. Four grafts including a LIMA-LAD, SVG-OM, SVG-Dx and Rad-OM1 were constructed to deliver flow to the distal myocardium. Mean flows in the LIMA-LAD, SVG-OM and SVG-Dx grafts were acceptable. However, mean Rad-OM1 graft flow measured 3.6 mL/min (PI: 12.7) signaling the need for revision of that graft. Following Rad-OM1 graft revision, mean graft flow improved to 18.3 mL/min (PI, 1.7) and was accompanied by a systolic/diastolic waveform.